Some Consequences of Spinal Cord Injury
The areas of the spinal cord commonly injured are the cervical spine (C4-C7), the mid thoracic spine and the lumbar spine (L1-L5). The notation C1, C7, T10, L1, L5 refer to the location of a specific vertebra in either the cervical, thoracic, or lumbar region of the spine.
Lesions at the cervical level C3 and above are not compatible with life, because the innervation of the diaphragm, necessary for breathing, arises from C4-5, and the intercostal muscles, also involved in respiratory movements, are innervated segmentally from the thoracic cord. A C3 lesion disconnects all of these muscles from the respiratory centre in the medulla, which is responsible for breathing.
Lesions of the lower cervical cord can cause major disability with lack of motor control of the upper limbs.
Spinal cord injuries in the lower lumbar vertebral segments usally affect the cauda equina. Cauda equina lesions are characterised by a loss of sensation in the saddle area and perineum, and loss or reduction of motor function in some distal muscles of the limbs. There may also be double incontinence and disturbances of sexual function.
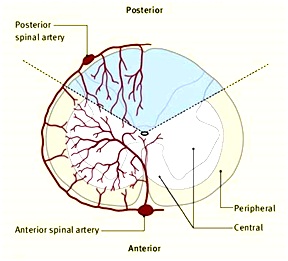
Lesions affecting prdominantly one side of the spinal cord results in the Brown-Sequard Syndrome, which has a characteristic combination of signs and symptoms.
|
Diagnosis of Spinal Cord Injury
Spinal cord injuries are caused by trauma to the spinal column (stretching, bruising, applying pressure, severing, laceration, lack of blood flow).
If the vertebral bones or intervertebral discs are damaged, the spinal cord to be punctured by a sharp fragment of bone.
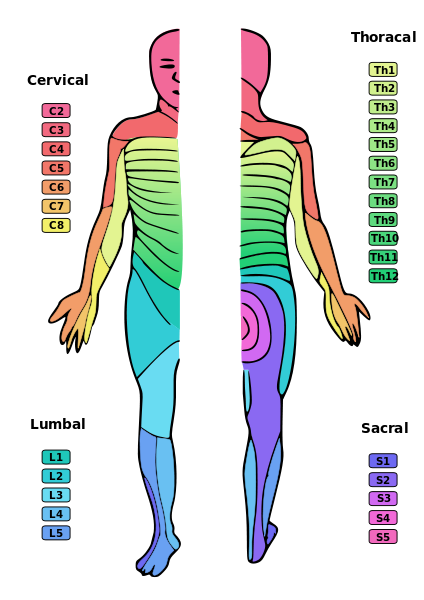
The usual signs and symptoms are the loss of sensation and of movement in dermatomes and myotomes below the level of the lesion.
When the paralysis and sensory loss affects only the lower limbs the condition is known as paraplegia, but if upper and lower limbs are affected the condition is quadriplegia.
Spinal shock is normal in the first few days to weeks and is characterised by a loss of reflex activity below the level of the lesion.
Later, muscles that have an intact innervation may become spastic and show increased reflex activity. Muscles that have lost their innervation atrophy and lack reflex activity. The reasons for these changes are discussed in the section on the Physiology of Muscle Tone in Chapter 4.
Other important functions affected by spinal cord injury are the control of the bladder and bowel.
|
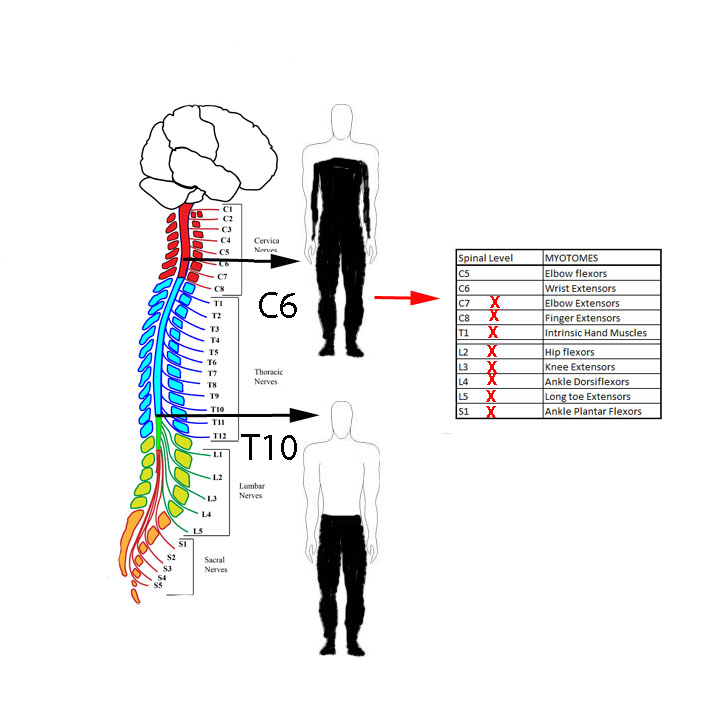
In patient with a C6 lesion the sensory loss is in the dermatomes below C6, and the motor loss is in myotomes below C6.
Thus there is some sensation in parts of the hands, particularly the thumb and index finger, but little motor control of the hands; but the patient can flex the elbows and extend the wrist.
In a patient with a T10 lesion there is sensory loss below the level of the umbilicus, and no motor control of the lower limbs. |